


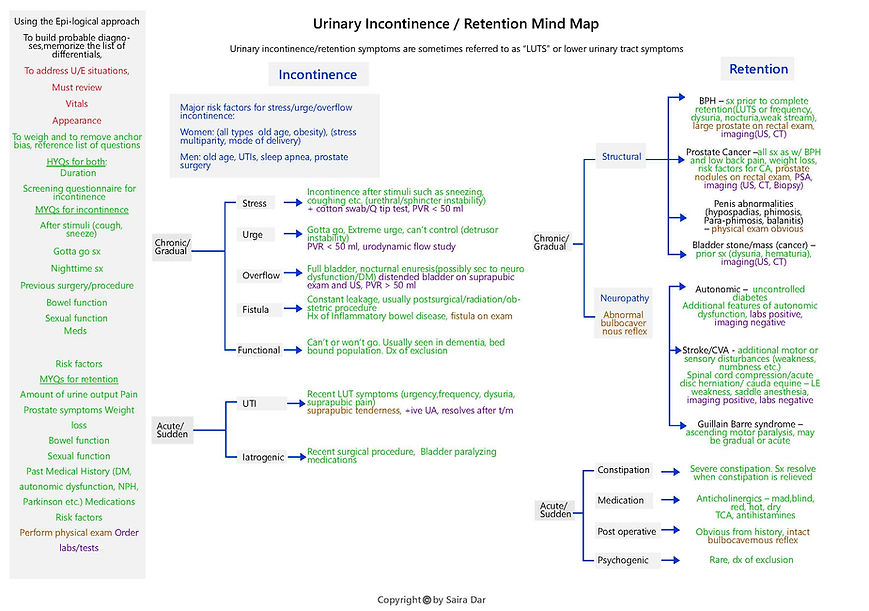
Patients may come in with urinary incontinence or retention that is of acute or chronic duration. There are a few differentials for each incontinence, and these differentials are listed based upon the first high yield question, which is duration. All differentials or probable diagnoses are grouped or based upon the initial high yield question. Medium yield questions are listed separately for each presentation.
Urgent/emergent situations include any differential that can be life or organ threatening, which occur in very few such situations, such as stroke, GBS, or severe infection. A patient’s appearance may indicate a level of discomfort which a clinician can use to assess for these situations, and vital signs must also be reviewed.
Weighing and removing anchor bias for incontinence involves questions about patterns or characteristics of incontinence, the past medical history which may point to risk factors, and additional associated symptoms that are listed on the mind map. The three most common causes of chronic incontinence are stress, overflow and urge incontinence, which are characteristically described as incontinence associated with coughing, sneezing, or any trigger which raises pelvic pressure, “gotta go” symptoms, and the inability to feel the urge. Patients usually are able to clearly explain their symptoms, such that a clinician can easily differentiate these diagnoses from one another. However, sometimes patients have multiple underlying pathologies, which leads them to present with overlapping features. A clinician can readily identify acute causes of incontinence because of the duration of symptoms and their association with concurrent conditions, such as UTI and/or iatrogenic events.
Weighing and removing anchor bias for retention involves questions about individual diagnoses on the list. Concerning diagnoses listed under chronic/gradual category, although several disease processes develop gradually, patients may not notice symptoms or seek attention until significant urinary obstruction occurs, and in this case a patient may present acutely. In these acute cases, a clinician’s careful exploration of a patient’s symptoms may reveal a gradual process. In most acute cases, patients may have a partial or intermittent retention. Asking about a constellation of symptoms related to individual diagnoses and looking for specific physical exam features can help a clinician narrow the differential diagnoses. Urinary retention may not be the initial presenting symptom for most differential diagnoses listed on this clinical mind map, but this may be an accompanying feature of a different chief complaint as a disease process progresses. Examples include Gillain Barre Syndrome, stroke, autonomic neuropathy, and constipation. In these cases of a different chief complaint, this clinical mind map may not be applicable. Appropriate labs and imaging tests help a clinician arrive at the final diagnosis.
A helpful mnemonic to memorize differentials for urinary incontinence is SOUFF-UI and a mnemonic to memorize differentials for chronic urinary retention are disorders of male reproductive system and BAGS